
MATERNAL MORTALITY: UNRAVELING THE INTERSECTIONAL WEB IN NIGERIA
AN OVERVIEW OF MATERNAL MORTALITY IN NIGERIA
Maternal mortality is a serious global health issue that is more prevalent in sub-Saharan Africa, contributing to about 70% of deaths in 2020, which is indicative of the gaps between the affluent and the non-affluent and unequal access to good health care (World Health Organization, 2023). Many countries have made strides in the fight against maternal mortality; however, with a global burden of over 20% (Ope, 2020), a maternal mortality ratio of 814 for every 100,000 live births and a combined total of about 34% of the world’s maternal mortality rates with India (WHO, 2015), Nigeria lags.
Research in Nigeria has indicated that women living in rural communities are predominately affected by poor maternal health outcomes in contrast to those in urban regions (Azuh et al., 2017) (Ibrahim, 2014), mainly due to a lack of access to professional health services (Okonofua et al., 2018), and therefore, many mothers count on the help of traditional birth attendants who are heavily utilised in rural communities (Esan et al., 2023). Furthermore, other studies suggest that the continual increase in maternal deaths is due to transportation barriers to health facilities, lack of prompt attendance by health professionals and poor decision-making in seeking timely care (Okonofua et al., 2018)(Yaya et al., 2018).
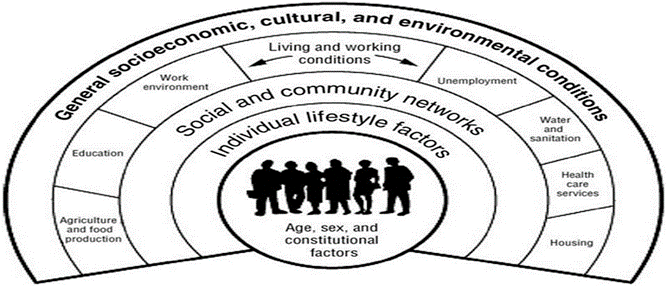
Introspectively, these issues can be linked to medical factors and, most importantly, non-medical factors (social determinants of health) (Figure 1) that play a massive role in determining inequalities in health (Cockerham, 2009, p. 78). Therefore, this article will analyse the intersectional factors contributing to maternal mortality in Nigeria while considering gender dynamics, socioeconomic factors, cultural and religious practices, regional disparities, and government policies. Investigating the gaps contributing to health disparities at all levels is imperative to recommend practical measures for change.
UNDERSTANDING GENDER DYNAMICS IN NIGERIA
Women have been subject to inequities in various societies forever, and this is still a reality for many women in Nigeria today. The societal expectation of women to bear children and take care of the home is overbearing, and it has affected their socioeconomic standing and access to financial resources, which, in turn, has affected their health outcomes (Borrell et al., 2014). Societal and cultural norms have allowed for the continual patriarchy, where some men dominate women, leaving them with no social or even personal autonomy. Over the years, many initiatives to empower the role of women in Nigerian societies have been enacted, including developing a Ministry for the Affairs of Women in 1995 and equity-promoting policies, such as “affirmative action” to improve socioeconomic outcomes and equity for women (Olonade et al., 2021). Nonetheless, all these initiatives and policies have proven fruitless, leaving many women in various societies at a disadvantage and facing multiple gender-discriminating stereotypes, regulating their access to socioeconomic advantages, which has affected their good health and well-being (Lan and Tavrow, 2017).
Most health outcomes are strongly influenced by gender (Krieger, 2003) (Sen and Ostlin, 2008), and women in Nigeria continue to face drastic maternal health outcomes due to imposing gender norms that keep widening the gaps in health inequities and inequalities.
SOCIOECONOMIC CHALLENGES: POVERTY AND EDUCATION
An individual’s socioeconomic standing can be devised as the significant origin of health inequality (Cockerham, 2007). Over 60% of women account for the overall poverty level in Nigeria (Ifeanyi et al., 2019), with women in rural communities accounting for most of the percentage. The high level of maternal deaths in Nigeria can be attributed to poverty and the low status of women across communities who have subpar educational attainment. The northern part of the country is more impoverished, and a correlation between educational attainment and maternal deaths has been seen (Meh et al., 2019).
Education is pivotal in influencing women’s behavioural decisions when seeking prompt health services (Yakubu et al., 2018); however, gaps in educational inequality persist in Nigeria. Lack of access to literacy and health education resources has left women in many communities with poor health outcomes. Cultural practices most prominent in the northern part of the country involve early marriage for girls who end up not attending educational institutions, which can influence maternal mortality (Meh et al., 2019). Many studies have shown an association between women’s educational attainment and maternal mortality ratios. For example, a study in sub-Saharan Africa suggests a strong relationship between education and maternal mortality (Alvarez et al., 2009). Recently, a study in Ethiopia (Borde, 2023) showed that women with poor educational attainment are more prone to socioeconomic inequalities.
CULTURAL AND RELIGIOUS PRACTICES IN NIGERIA
Cultural practices are deeply rooted in many communities of Nigeria, especially in rural communities where women prefer to deliver their babies with the help of a traditional birth attendant who has gained a level of acceptance from living in the same community. Due to transportation and financial barriers, most women cannot access skilled birth attendants. Therefore, they have to rely solely on the expertise of traditional birth attendants who still need formal education training (Garces et al., 2019). Early marriage practices for young girls, especially in the northern culture, leading to painful and complicated pregnancies, are a contributor to maternal deaths. Additionally, religious practices in some areas where married women are prohibited by their husbands from seeing a skilled male professional during or after pregnancy have contributed to their deficient health outcomes. Families in some parts of the country are strictly traditional and do not utilize modern healthcare.
All these practices have proven detrimental to maternal mothers, and existing structural disparities have perpetuated the continual of such practices amongst populations.
REGIONAL DISPARITIES
Nigeria, the most populous country in Africa, has six geopolitical zones, with North and South as its major regions (Adebowale et al., 2012). There’s a distinct difference if we compare the population status of educational accomplishments and the accessibility of health facilities between these regions (Henry V. Doctor et al., 2012). Consequently, maternal mortality rates are disproportionally distributed, with the highest burden seen in the northern states (Meh et al., 2019), which is attributed to illiteracy and underserved and underdeveloped health facilities (Alabi et al., 2014). It has been reported that the rates of maternal deaths seen in northern states are second-rate worldwide (Henry Victor Doctor et al., 2012). Most of these mortality cases go unreported because they happen in homes, and there is poor data reporting practice across healthcare facilities (Sharma et al., 2017). Compared to the South, most women in the North do not utilise health facilities but are put to bed in their homes (Ononokpono and Odimegwu, 2014). A higher burden of maternal deaths is seen in the North due to the common practice of early marriages (Henry Victor Doctor et al., 2012). Conversely, women have been associated with the use of traditional contraception, which is mainly attributed to maternal mortality in the South (Meh et al., 2019). All these factors have contributed to outcome imbalance across regions in Nigeria.
GOVERNMENT POLICIES AND INTERVENTIONS
The Abuja Declaration in 2001 emerged as a beacon of hope through the government’s effort to boost health financing, and as a result, maternal deaths dropped from 856 to 512 per live births between 2015 and 2020 (Adegoke et al., 2022). Several programs, policies and interventions have been implemented ever since. For example, a maternal cash transfer programme, “SURE-P MCH” (Onwujekwe et al., 2020), which ran from 2012 to 2015 to facilitate efficient services for pregnant mothers was plagued with challenges (Oduenyi et al., 2019). As a result, it was not sustained to achieve significant outcomes. Several other government strategies, like the “free maternal and child health program” (Onwujekwe et al., 2019) and health insurance schemes, have shown varying outcomes across different locations in Nigeria (Mao et al., 2023). Consequently, maternal mortality is still on the rise today due to the government’s continual dismissal of addressing health as a fundamental human right through a lack of increased financing for health and strengthening of health systems, leaving thousands of women with poor health outcomes in Nigeria.
CONCLUSION AND RECOMMENDATIONS
Even though maternal deaths are preventable with strategic schemes, we can see the disturbing rate in Nigeria stems from intersectional factors that have been weaved into gender inequalities, socioeconomic factors, cultural and religious practices and ineffective governmental interventions and policies. Policymakers must not only increase accessibility to health and revitalise health systems delivery but also look into the political, social, and environmental factors as core contributors to inequities (Heise et al., 2019). Finally, with the recommendations below, the government must take comprehensive action using an intersectional lens and a multisectoral approach to save women’s lives in Nigeria.
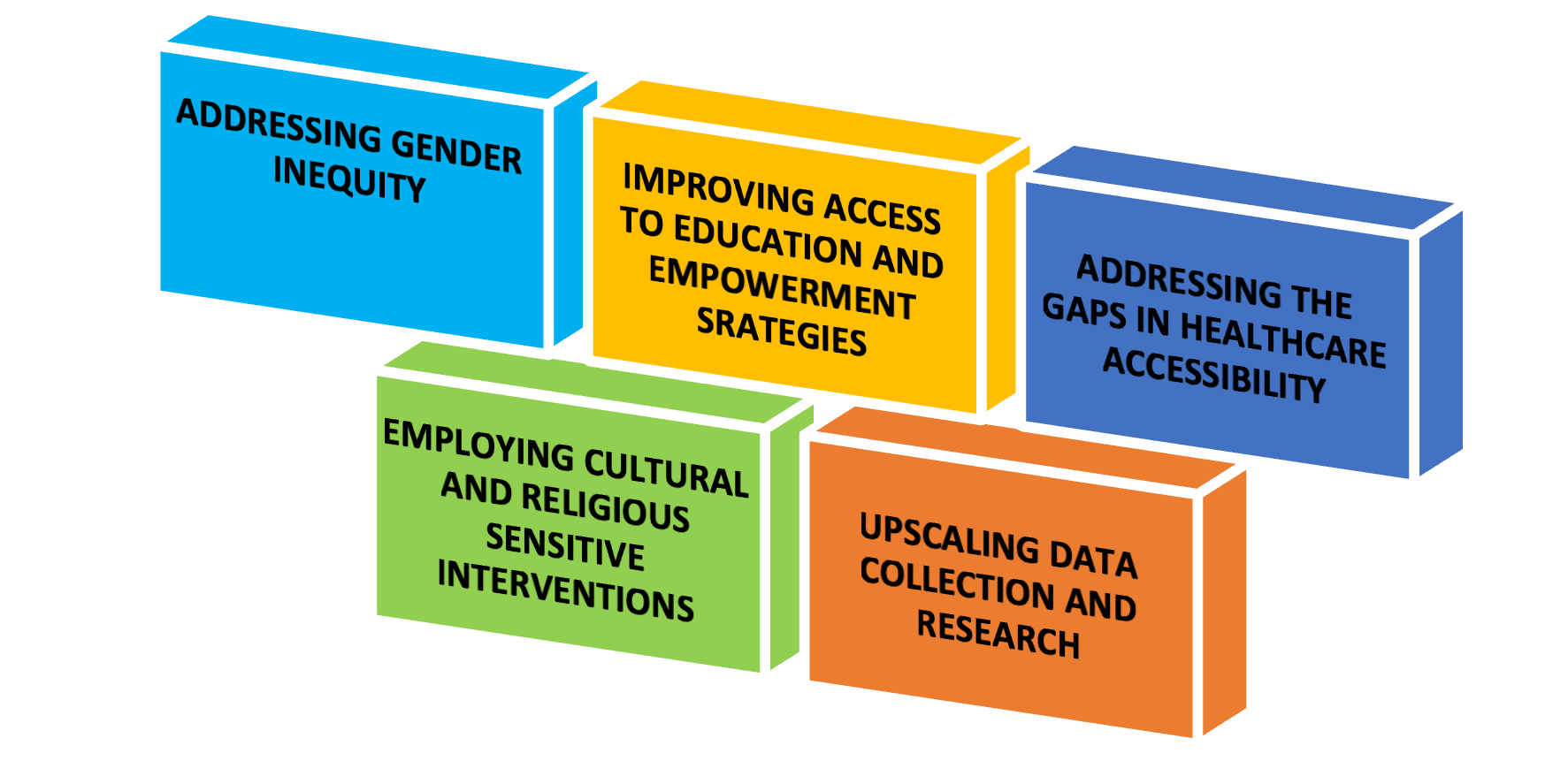
RECOMMENDATIONS
- Addressing gender inequity in Nigeria: The poor health outcomes of women in Nigeria can be attributed to gender inequity, which is ingrained in societies. It is imperative to prioritise equity to increase the status and freedom of women and break down existing barriers. To achieve this, we must first address the issue of poverty and low levels of education.
- Improving access to education and empowerment strategies for women: From the above findings, we can deduce the importance of women’s educational attainment, which can influence health decision-making and reduce maternal mortality (Koch et al., 2012). Women’s empowerment through education can positively impact their decision-making capacity (Dimbuene et al., 2018), especially in a patriarchal society like Nigeria, where some women lack autonomy. Reinforcing the legal age for marriage can be a strategy to increase school attendance for girls (Meh et al., 2019). Cash transfer programs can empower women, increasing their decision-making capacity and health outcomes. This can be seen in Brazil’s success (de Brauw et al., 2014) and can be replicated by carefully considering intersecting factors to achieve positive health outcomes for women in Nigeria.
- Addressing gaps in healthcare accessibility in Nigeria: Deploying skilled professionals, especially in rural areas and strengthening health systems’ service capacities, especially primary healthcare centres, as the first contact for women in communities. Reducing corruption in the healthcare system can improve maternal health outcomes (Lan and Tavrow, 2017). Increasing health coverage can be pivotal in curbing maternal deaths, as evidenced by a recent study in Nigeria (Mao et al., 2023). Furthermore, research has shown that many interventions primarily aim to address the proximal determinants of health without giving much attention to addressing distal factors contributing to maternal health outcomes in Nigeria (Nasir et al., 2022). Therefore, we must consider the structural conditions of living and work for people and social categorisation (Dahlgren and Whitehead, 1991). Lastly, regional disparities must be addressed to achieve proportional maternal health outcomes and universal coverage across various regions.
- Cultural and religious sensitive healthcare interventions: Nigeria is a multi-ethnic country with many women in communities and regions engrossed in cultural, traditional and religious practices. With that in mind, policymakers need to Initiate healthcare interventions through community involvement and empowerment strategies to assess populations’ specific needs, which can be vital in understanding cultural and religious nuances to develop effective Interventions that improve women’s health and quality of life.
- Upscaling health data collection and research in Nigeria: Accurate monitoring and data collection practices at facility levels to track maternal mortality rates to improve outcomes (Henry Victor Doctor et al., 2012). Research around maternal health outcomes is necessary because several studies show that utilising research evidence can go a long way in boosting health policy development and implementation (Campbell et al., 2009) (Innvær et al., 2002). It has been found that foreign researchers accrue over a third of maternal and neonatal health research in Nigeria (Nasir et al., 2022); therefore, local research must be upscaled to achieve context-specific goals.
REFERENCES
Adebowale, A.S., Yusuf, B.O., Fagbamigbe, A.F., 2012. Survival probability and predictors for woman experience childhood death in Nigeria: “analysis of North-South differentials.” BMC Public Health 12, 430. https://doi.org/10.1186/1471-2458-12-430
Adegoke, Y.O., Mbonigaba, J., George, G., 2022. Macro-economic determinants, maternal and infant SDG targets in Nigeria: Correlation and predictive modeling. Front. Public Health 10, 999514. https://doi.org/10.3389/fpubh.2022.999514
Alabi, O., Doctor, H.V., Jumare, A., Sahabi, N., Abdulwahab, A., Findley, S.E., Abubakar, S.D., 2014. Health & demographic surveillance system profile: the Nahuche Health and Demographic Surveillance System, Northern Nigeria (Nahuche HDSS). Int. J. Epidemiol. 43, 1770–1780. https://doi.org/10.1093/ije/dyu197
Alvarez, J.L., Gil, R., Hernández, V., Gil, A., 2009. Factors associated with maternal mortality in Sub-Saharan Africa: an ecological study. BMC Public Health 9, 462. https://doi.org/10.1186/1471-2458-9-462
Borde, M.T., 2023. Geographical and Socioeconomic Inequalities in Maternal Mortality in Ethiopia. Int. J. Soc. Determinants Health Serv. 53, 282–293. https://doi.org/10.1177/27551938231154821
Borrell, C., Palència, L., Muntaner, C., Urquía, M., Malmusi, D., O’Campo, P., 2014. Influence of Macrosocial Policies on Women’s Health and Gender Inequalities in Health. Epidemiol. Rev. 36, 31–48. https://doi.org/10.1093/epirev/mxt002
Campbell, D.M., Redman, S., Jorm, L., Cooke, M., Zwi, A.B., Rychetnik, L., 2009. Increasing the use of evidence in health policy: practice and views of policymakers and researchers. Aust. N. Z. Health Policy 6, 21. https://doi.org/10.1186/1743-8462-6-21
Cockerham, W.C., 2009. The New Blackwell Companion to Medical Sociology. John Wiley & Sons, Incorporated, Hoboken, UNITED KINGDOM.
Cockerham, W.C., 2007. Health lifestyles and the absence of the Russian middle class. Social. Health Illn. 29, 457–473. https://doi.org/10.1111/j.1467-9566.2007.00492
De Brauw, A., Gilligan, D.O., Hoddinott, J., Roy, S., 2014. The Impact of Bolsa Família on Women’s Decision-Making Power. World Dev. 59, 487–504. https://doi.org/10.1016/j.worlddev.2013.02.003
Dahlgren, Göran and Margaret Whitehead. 1991. Policies and Strategies to Promote Social Equity in Health. Stockholm: Institute of Future Studies.
Dimbuene, Z.T., Amo-Adjei, J., Amugsi, D., Mumah, J., Izugbara, C.O., Beguy, D., 2018. WOMEN’S EDUCATION AND UTILIZATION OF MATERNAL HEALTH SERVICES IN AFRICA: A MULTI-COUNTRY AND SOCIOECONOMIC STATUS ANALYSIS. J. Biosoc. Sci. 50, 725–748. https://doi.org/10.1017/S0021932017000505
Doctor, Henry V., Findley, S.E., Ager, A., Cometto, G., Afenyadu, G.Y., Adamu, F., Green, C., 2012. Using community-based research to shape the design and delivery of maternal health services in Northern Nigeria. Reprod. Health Matters 20, 104–112. https://doi.org/10.1016/S0968-8080(12)39615-8
Doctor, Henry Victor, Olatunji, A., Findley, S.E., Afenyadu, G.Y., Abdulwahab, A., Jumare, A., 2012. Maternal mortality in northern Nigeria: findings of a health and demographic surveillance system in Zamfara State, Nigeria. Trop. Doct. 42, 140–143. https://doi.org/10.1258/td.2012.120062
Esan, D.T., Ayenioye, O.H., Ajayi, P.O., Sokan-Adeaga, A.A., 2023. Traditional birth attendants’ knowledge, preventive and management practices for postpartum haemorrhage in Osun State, Southwestern Nigeria. Sci. Rep. 13, 12314. https://doi.org/10.1038/s41598-023-39296-y
Garces, A., McClure, E.M., Espinoza, L., Saleem, S., Figueroa, L., Bucher, S., Goldenberg, R.L., 2019. Traditional birth attendants and birth outcomes in low-middle income countries: A review. Semin. Perinatol., Current State of Health of Women and Children in Low and Middle Income Countries 43, 247–251. https://doi.org/10.1053/j.semperi.2019.03.013
Heise, L., Greene, Margaret E, Opper, N., Stavropoulou, M., Harper, C., Nascimento, M., Zewdie, D., Darmstadt, G.L., Greene, Margaret Eleanor, Hawkes, S., Heise, L., Henry, S., Heymann, J., Klugman, J., Levine, R., Raj, A., Rao Gupta, G., 2019. Gender inequality and restrictive gender norms: framing the challenges to health. The Lancet 393, 2440–2454. https://doi.org/10.1016/S0140-6736(19)30652-X
Ifeanyi, O., Anthony, N., Prisca, I., 2019. Poverty among Women in Nigeria–Psychological and Economic Perspective: A Study Based On South West, Nigeria. Int. J. Bus. Manag. 14, p90. https://doi.org/10.5539/ijbm.v14n11p90
Innvær, S., Vist, G., Trommald, M., Oxman, A., 2002. Health policy-makers’ perceptions of their use of evidence: a systematic review. J. Health Serv. Res. Policy 7, 239–244. https://doi.org/10.1258/135581902320432778
Koch, E., Thorp, J., Bravo, M., Gatica, S., Romero, C.X., Aguilera, H., Ahlers, I., 2012. Women’s Education Level, Maternal Health Facilities, Abortion Legislation and Maternal Deaths: A Natural Experiment in Chile from 1957 to 2007. PLoS ONE 7, e36613. https://doi.org/10.1371/journal.pone.0036613
Krieger, N., 2003. Genders, sexes, and health: what are the connections–and why does it matter? Int. J. Epidemiol. 32, 652–657. https://doi.org/10.1093/ije/dyg156
Lan, C.-W., Tavrow, P., 2017. Composite measures of women’s empowerment and their association with maternal mortality in low-income countries. BMC Pregnancy Childbirth 17, 337. https://doi.org/10.1186/s12884-017-1492-4
Mao, W., Watkins, D., Sabin, M.L., Huang, K., Langlois, E., Ogundeji, Y., Fogstad, H., Schäferhoff, M., Yamey, G., Ogbuoji, O., 2023. Effects of public financing of essential maternal and child health interventions across wealth quintiles in Nigeria: an extended cost-effectiveness analysis. Lancet Glob. Health 11, e597–e605. https://doi.org/10.1016/S2214-109X(23)00056-6
Meh, C., Thind, A., Ryan, B., Terry, A., 2019. Levels and determinants of maternal mortality in northern and southern Nigeria. BMC Pregnancy Childbirth 19, 417. https://doi.org/10.1186/s12884-019-2471-8
Nasir, N., Aderoba, A.K., Ariana, P., 2022. Scoping review of maternal and newborn health interventions and programmes in Nigeria. BMJ Open 12, e054784. https://doi.org/10.1136/bmjopen-2021-054784
Oduenyi, C., Ordu, V., Okoli, U., 2019. Assessing the operational effectiveness of a maternal and child health (MCH) conditional cash transfer pilot programme in Nigeria. BMC Pregnancy Childbirth 19, 298. https://doi.org/10.1186/s12884-019-2418-0
Okonofua, F., Ntoimo, L., Ogungbangbe, J., Anjorin, S., Imongan, W., Yaya, S., 2018. Predictors of women’s utilization of primary health care for skilled pregnancy care in rural Nigeria. BMC Pregnancy Childbirth 18, 106. https://doi.org/10.1186/s12884-018-1730-4
Olonade, O.Y., Oyibode, B.O., Idowu, B.O., George, T.O., Iwelumor, O.S., Ozoya, M.I., Egharevba, M.E., Adetunde, C.O., 2021. Understanding gender issues in Nigeria: the imperative for sustainable development. Heliyon 7, e07622. https://doi.org/10.1016/j.heliyon.2021.e07622
Ononokpono, D.N., Odimegwu, C.O., 2014. Determinants of Maternal Health Care Utilization in Nigeria: a multilevel approach. Pan Afr. Med. J. 17, 2. https://doi.org/10.11694/pamj.supp.2014.17.1.3596
Onwujekwe, O., Ensor, T., Ogbozor, P., Okeke, C., Ezenwaka, U., Hicks, J.P., Etiaba, E., Uzochukwu, B., Ebenso, B., Mirzoev, T., 2020. Was the Maternal Health Cash Transfer Programme in Nigeria Sustainable and Cost-Effective? Front. Public Health 8, 582072. https://doi.org/10.3389/fpubh.2020.582072
Onwujekwe, O., Obi, F., Ichoku, H., Ezumah, N., Okeke, C., Ezenwaka, U., Uzochukwu, B., Wang, H., 2019. Assessment of a free maternal and child health program and the prospects for program re-activation and scale-up using a new health fund in Nigeria. Niger. J. Clin. Pract. 22, 1516–1529. https://doi.org/10.4103/njcp.njcp_503_18
Ope, B.W., 2020. Reducing maternal mortality in Nigeria: addressing maternal health services’ perception and experience. J. Glob. Health Rep. 4, e2020028. https://doi.org/10.29392/001c.12733
Sen, G., Ostlin, P., 2008. Gender inequity in health: why it exists and how we can change it. Glob. Public Health 3 Suppl 1, 1–12. https://doi.org/10.1080/17441690801900795
Sharma, V., Brown, W., Kainuwa, M.A., Leight, J., Nyqvist, M.B., 2017. High maternal mortality in Jigawa State, Northern Nigeria estimated using the sisterhood method. BMC Pregnancy Childbirth 17, 163. https://doi.org/10.1186/s12884-017-1341-5
World Health Organization, 2023. Maternal mortality [WWW Document]. URL https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (accessed 12.26.23).
World Health Organization, 2015. Trends in Maternal Mortality: 1990 to 2015 – Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division – World | ReliefWeb [WWW Document]. URL https://reliefweb.int/report/world/trends-maternal-mortality-1990-2015-estimates-who-unicef-unfpa-world-bank-group-and (accessed 12.26.23).
Yaya, S., Okonofua, F., Ntoimo, L., Kadio, B., Deuboue, R., Imongan, W., Balami, W., 2018. Increasing women’s access to skilled pregnancy care to reduce maternal and perinatal mortality in rural Edo State, Nigeria: a randomized controlled trial. Glob. Health Res. Policy 3, 12. https://doi.org/10.1186/s41256-018-0066-y
Munira Musa Ladan
Executive Director
Elkheir Healthcare Foundation